

Pediatric Heart Topic
Pediatric Heart Topic
Transplants

The AATS listed an article from the Journal of Thoracic and Cardiovascular Surgery published on December 1, 2022 that looked at 427 cases of pediatric patients that needed a heart transplant with renal insufficiency. The results indicate an improvement in waitlist time and post-transplant mortality rates decreased when the patient was listed for dual-organ heart and kidney transplant.
Survival in pediatric HTx has improved in recent decades due to advancements in management and organ allocation. The latest report by the Organ Procurement and Transplantation Network indicates a median survival of approximately 94% at 1 year and 85% at 5 years after transplantation.
1 Despite these positive outcomes, renal insufficiency often accompanies end-stage heart failure, complicating decisions regarding the course of treatment.2 Renal insufficiency poses a serious risk factor for waitlist and post-transplantation mortality, and several studies have demonstrated that renal dysfunction often progresses after HTx.2, 3, 4

This is an interesting topic of research.
Something I’ve learned from being married to a Pediatric Nurse is that research is important; without her research during the pregnancy with our twins, the outcome for Grace would have been different. Grace has taught me the balanced fragility of life with strength to a more significant level than I’ve ever understood. Her infradiaphragmatic TAPVR, two open heart surgeries while developing Protein Losing Enteropathy along the way; her smiles and laughter are genuine, though the journey is far from over; as is the research into the effectiveness of transplant listings with associated mortality outcomes as the article notes:
Still, the lack of national overview with a pediatric population examining HKTx from listing limits the validity of these studies. Therefore, the purpose of this study is to analyze HKTx listing outcomes as opposed to isolated HTx listing for pediatric candidates with renal insufficiency to better recommend and evaluate treatment strategies for these patients.
If you’re curious, here’s an off topic reference for two types of TAPVR:
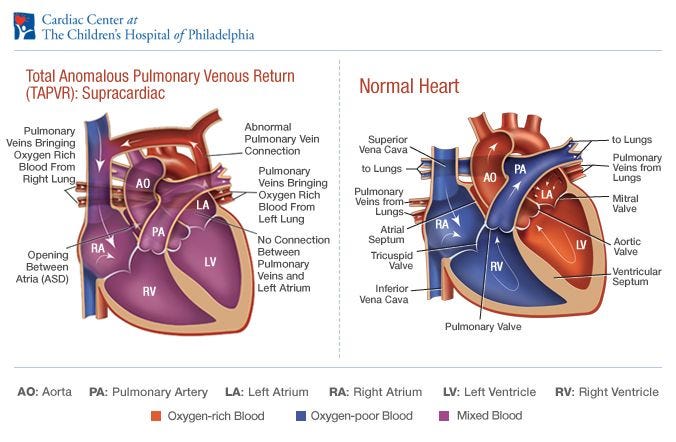

Grace’s TAPVR went through her liver, just a bit lower of a route than the infracardic. The crazy bit, is how resilient physiological development can be as it finds a path to survive in the most creative ways. As Grace developed her Inferior Vena Cava clot, her body made a collateral vein that connected to the heart to get that needed circulation, though inefficient. Hence the second open heart surgery, now we are chasing PLE.
My heart is with all who may be standing near a CICU with a heart warrior, it’s a difficult place of anticipation.

Flowers grow in harsh places.
Ojibwe: Compassion all over the world